
Pseudodementia Explained: The Condition Often Mistaken For Dementia
Prepared by Dr. Aldona Šileikaitė
Introduction
There is little doubt today that populations around the world are aging. Advances in modern medicine have helped extend life expectancy, while lower birth rates, migration patterns and other demographic changes continue to reshape societies. These shifts are visible not only in statistics, but also in everyday medical practice, where elderly patients increasingly make up a large proportion of doctor visits.
Family members often notice the first worrying signs. An older relative may remember childhood events in vivid detail yet struggle to recall what happened earlier that same day. At first, these moments can seem harmless or even touching, especially when they lead to stories and shared memories. Over time, however, the situation may become more concerning. Some elderly people begin getting confused in familiar surroundings, forgetting where they are going or becoming lost outside the home. In advanced stages, independence gradually disappears, higher cognitive interests fade and continuous care becomes necessary.
Dementia is a condition characterized by progressive loss of cognitive functions. Diagnosis is based not only on clinical evaluation but also on standardized diagnostic scales and cognitive testing. In some cases, however, objective assessment becomes difficult because mood disorders can produce symptoms that resemble dementia. Severe depressive episodes and dementia may both involve memory impairment, slower thinking, apathy and reduced motivation.
This overlap has led to the concept of pseudodementia, a condition in which cognitive symptoms mimic dementia but arise primarily from psychiatric causes rather than neurodegenerative disease. Pseudodementia is often discussed alongside normal aging, mild cognitive impairment (MCI) and dementia because distinguishing between these states can be clinically challenging.
Pseudodementia
The term pseudodementia first appeared in medical literature in 1961 to describe cognitive disorders that closely resemble dementia symptoms without evidence of a neurodegenerative process. Two components are necessary for this diagnosis: the dementia-like presentation involving various cognitive impairments, and the “pseudo” component, meaning the absence of underlying degenerative dementia.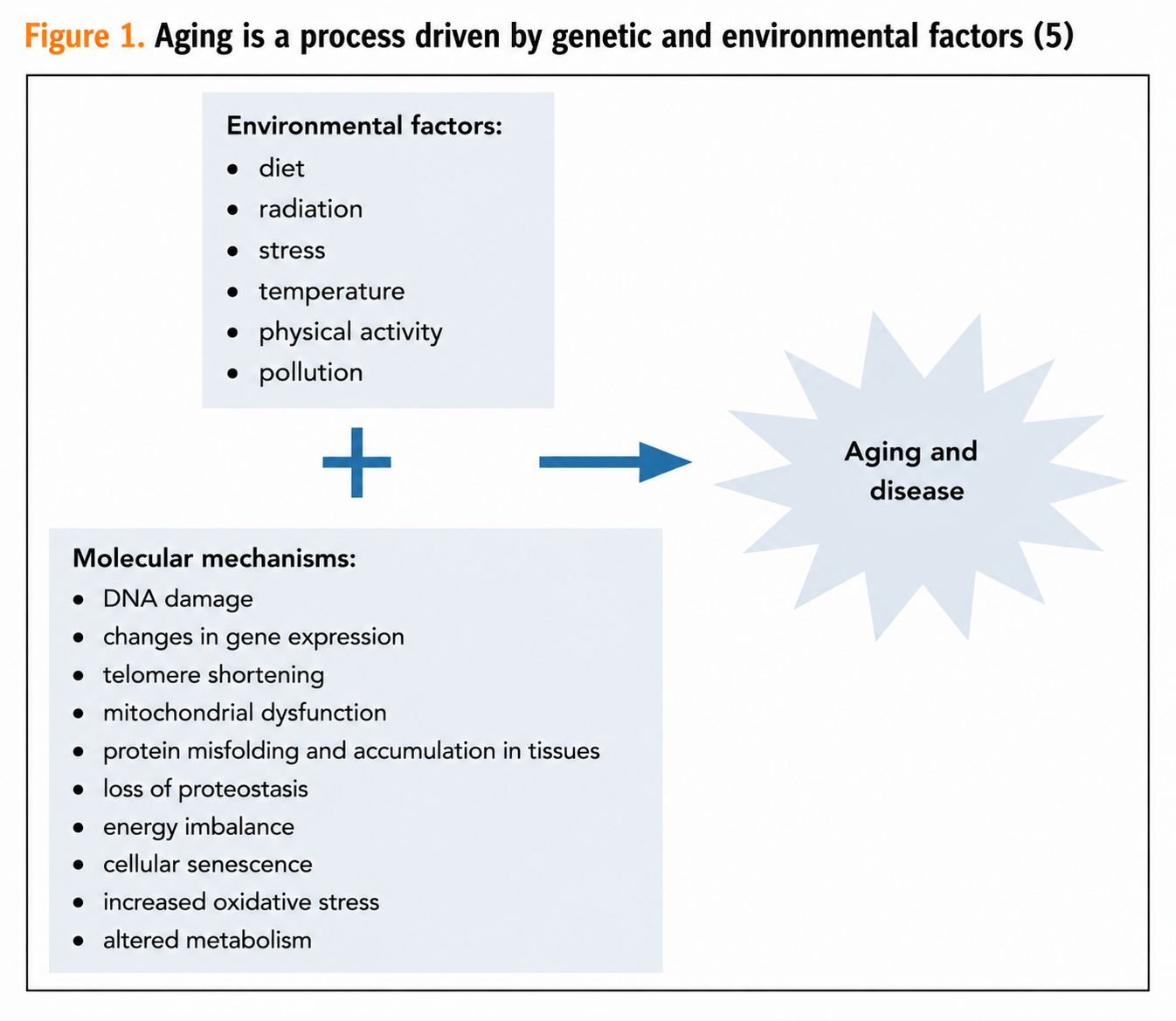
Pseudodementia
Pseudodementia is a descriptive term. It is especially important in cases of depression in older people, where it is necessary to correctly distinguish symptoms of dementia from symptoms of depression. In clinical practice, this is particularly relevant because:
● cognitive changes in older people often blur the boundary between normal aging and the early signs of pseudodementia; ● depression is frequently accompanied by cognitive impairment, which may be quite severe; ● symptoms of certain neurological diseases overlap with symptoms of depression; ● dementia may coexist together with depression.
Among cognitive functions, memory is affected the most. This is associated with slower reactions, reduced ability to retain new information, and weaker encoding of information compared with healthy individuals. In addition, work capacity decreases, speech recognition deteriorates, and reading and writing tasks are performed worse (1).
Pseudodementia is considered a reversible condition that improves once the underlying disease is treated. It is most commonly associated with major depressive episodes, bipolar disorder, schizophrenia or Ganser syndrome. Key differences between pseudodementia and dementia include a clearer onset of symptoms, more rapid deterioration, relatively preserved attention and concentration, and minimal effort by the patient to compensate for symptoms.
There is ongoing debate in the scientific literature regarding whether pseudodementia symptoms are truly fully reversible or whether pseudodementia itself may represent a risk factor for dementia later in life. Some evidence suggests that depression may act as a prodromal stage of Alzheimer’s disease and vascular dementia (2).
Normal Aging
Normal aging is associated with structural and neurophysiological changes in the brain, as well as gradual decline in cognitive functions. Due to age-related changes, brain cortical tissue shrinks, particularly in the frontal cortex and hippocampus. Aging is also associated with atrophy of the frontal, parietal, temporal and occipital lobes, together with white matter changes. Studies have shown that individuals with mild cognitive impairment lose more brain tissue over time in cortical gray matter and in the frontal and occipital lobes (3).
In addition, the aging process is strongly influenced by environmental conditions, physical activity and genetics. It has been estimated that heredity determines approximately 25% of lifespan. Individual genes and their combinations have been studied extensively, most of them localized on chromosome 3. The most widely studied genes are APOE and FOXO3A and their variants (4). On a biological level, genes interact with environmental factors, leading to oxidative stress, telomere shortening, inflammatory processes and other mechanisms that eventually result in cell damage and death. Considerable attention has also been directed toward mitochondria, which are responsible for maintaining cellular energy balance. The interaction between environmental and genetic factors is illustrated in Figure 1 (5).
Mild Cognitive Impairment
Mild cognitive impairment (MCI) is considered an intermediate stage between normal aging and dementia. This disorder is diagnosed in individuals whose daily functioning remains preserved but who complain of worsening memory and slower thinking or work pace. The European Alzheimer’s Disease Consortium criteria are commonly used for diagnosis:
● complaints of cognitive impairment expressed by the patient or relatives; ● reports from the patient or relatives indicating worsening cognitive function over recent years; ● cognitive impairments confirmed during clinical evaluation; ● impairments that do not interfere with daily functioning but may complicate more complex activities; ● absence of dementia.
Amnestic and non-amnestic forms of MCI are distinguished. The amnestic type, characterized predominantly by memory impairment, has the highest likelihood of progressing to Alzheimer’s disease (6). Scales of normal aging and pathological cognitive changes are shown in Figure 2.
Dementia
According to the World Health Organization (WHO), approximately 47.5 million people worldwide live with dementia, and around 7.7 million new cases are diagnosed every year. Alzheimer’s disease is the most common cause of dementia, accounting for 60–70% of all cases (11).
Dementia is usually associated with older age, although in some cases younger individuals may also be affected. This condition is known as early-onset dementia and is diagnosed when symptoms occur before the age of 65. The prevalence is estimated at 42.4–54 cases per 100,000 people. Unlike other forms of dementia, early-onset dementia often initially affects cognitive functions more strongly than memory itself. Early symptoms may also be overlooked and attributed to stress or fatigue (7).
Dementia is a clinical syndrome characterized by acquired impairment of cognitive functions without disturbances of consciousness. According to DSM-V, diagnostic criteria include:
● significant decline in cognitive functioning compared with a previous level in one or more domains such as attention, executive function, learning and memory, language or cognition; ● cognitive deficits that interfere with daily activities; ● symptoms that are not explained exclusively by delirium; ● cognitive deficits that cannot be better explained by another mental disorder (8).
WHO Facts About Dementia
Dementia represents a major global public health issue. WHO highlights several key facts:
● dementia is not a normal part of aging; ● the number of people living with dementia worldwide reached 47.5 million in 2015, with 58% living in low- and middle-income countries. By 2050, prevalence is projected to increase by 71%; ● approximately 7.7 million new dementia cases are diagnosed each year, equivalent to one new case every 4 seconds; ● dementia treatment creates a major burden for healthcare systems because of rising prevalence and associated costs. Current estimated costs reach 604 billion USD annually and are expected to continue increasing; ● caregivers of people with dementia experience substantial physical, emotional and financial strain and therefore require comprehensive support; ● key principles of dementia care include early diagnosis, optimization of physical health and well-being, treatment of behavioral and psychological symptoms, and long-term support for caregivers; ● people with dementia are often deprived of freedoms and rights available to others, and physical or chemical restraint measures are still commonly used in care institutions; ● education and awareness at all levels of society are necessary to reduce stigma and improve quality of life for both patients and caregivers; ● further scientific research is needed to develop more effective treatments; ● dementia is considered a major public health priority, including efforts to promote dementia-friendly societies and invest in dementia research (11).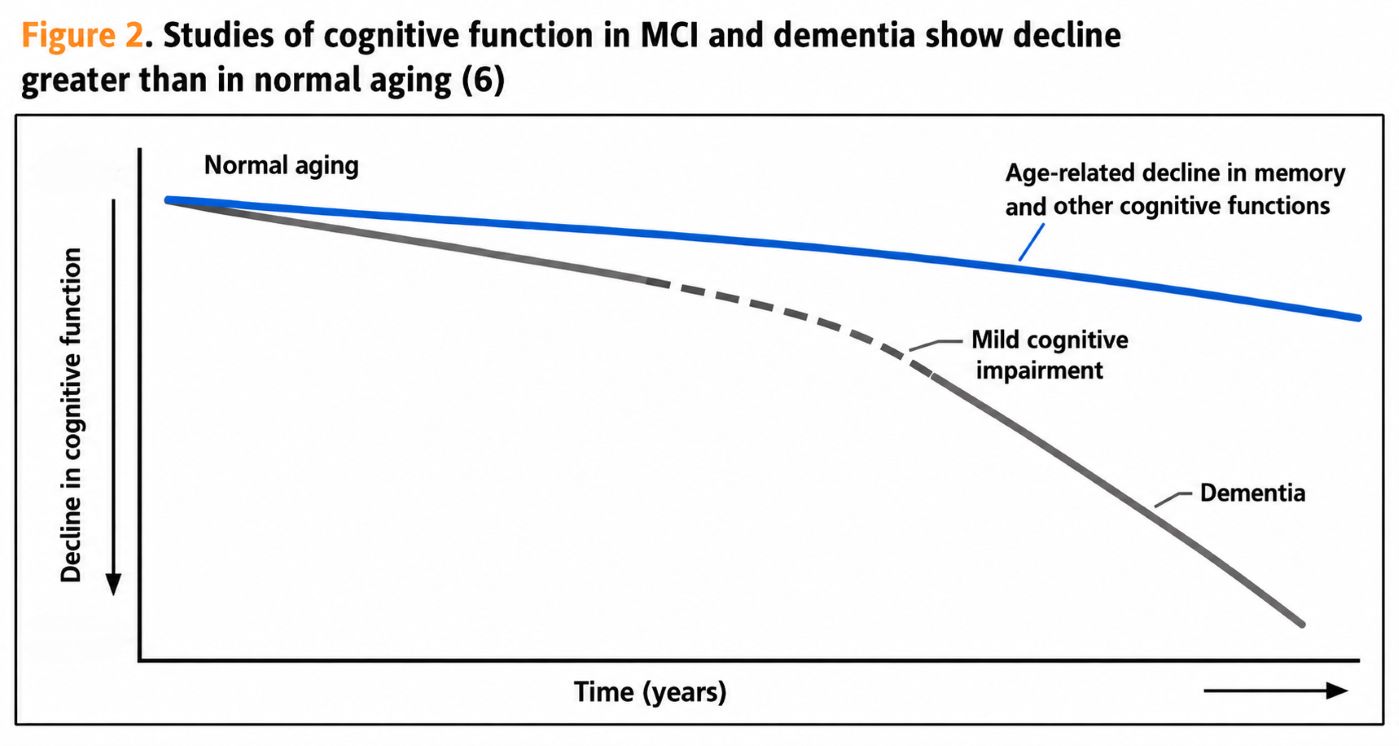
Non-pharmacological Treatment Methods
In addition to pharmacological treatment with cholinesterase inhibitors, neuroprotective agents, dietary supplements and other medications, scientific literature increasingly discusses non-pharmacological treatment approaches. The main goal of these methods is to stimulate brain activity, reduce the progression of dementia, preserve the patient’s dignity and decrease stress experienced by both patients and caregivers.
Some psychosocial interventions also help patients perceive themselves not only as individuals with illness. Encouraging memories and discussions about earlier life experiences may help restore former roles, emotions and a sense of identity, which can positively affect emotional well-being. Family members also benefit from learning more about the patient’s personality and life history.
Storytelling methods are frequently used in dementia care, allowing patients to identify with certain events or episodes from stories. In couples, the life story method is often applied, where the healthy partner recounts their shared experiences to the patient while using visual materials such as photographs, videos or audio recordings (9).
These psychosocial interventions are also described as simulated presence therapy. The method was developed empirically after observations that dementia patients visited by relatives in nursing homes appeared less agitated and smiled more frequently. Scientifically, this approach was first described in 1995 (10).
Conclusion
As populations continue to age, there is a growing need to better understand the mechanisms of normal aging and syndromes associated with acquired cognitive impairment. In clinical practice, it is not always easy to distinguish whether memory problems still fall within the limits of normal aging, whether they are masked by an undiagnosed mood disorder, or whether they already represent a clear dementia syndrome.
There are hypotheses suggesting that some lost cognitive functions may potentially be partially restored through stimulation of brain activity and activation of memories. Perhaps future scientific advances will discover ways to activate remaining synaptic connections and restore at least some degree of independence to patients with dementia. At present, however, psychosocial interventions already appear to help reduce distress and improve emotional well-being for both patients and their relatives.Publication "Internistas" (163)
Reference list in the editorial office
