
Sinus Tachycardia: A Physiological Response or a Pathological Condition?
Introduction
Heart rate (HR) is one of the most commonly measured vital signs in clinical practice. It influences myocardial metabolism and cardiac output (1). In adults, tachycardia is generally defined as a heart rate exceeding 100 beats per minute. Tachycardia most commonly develops as a normal physiological response to physical exertion or stress. However, tachycardia occurring at rest requires greater attention and investigation of its underlying causes. In individuals with cardiovascular disease, tachycardia may contribute to myocardial infarction, hypotension, peripheral hypoperfusion, cardiomyopathy, and serious symptoms such as chest pain, weakness, syncope, and dizziness. It can also reduce cardiac output, precipitate cardiac arrest, and increase the risk of death (2).
Tachycardia can be classified into sinus tachycardia (physiological and pathological), postural orthostatic tachycardia syndrome (POTS), supraventricular tachycardias (atrial tachycardia, atrioventricular [AV] nodal re-entry tachycardia), atrial flutter with rapid ventricular response, atrial fibrillation with rapid ventricular response, junctional tachycardia, and ventricular tachycardia.
Sinus tachycardia is the most common type encountered in clinical practice. It differs from the other forms of tachycardia because, in most cases, it is physiological and related to activation of the sympathetic nervous system and the release of catecholamines, for example during emotional stress, physical activity, pain, or psychological stress. This type of tachycardia usually resolves once the underlying trigger, such as stress, pain, or fever, is removed. However, a small proportion of patients experience persistent sinus tachycardia. When no specific etiological factors can be identified, the condition is considered pathological and may require treatment.
Clinical Manifestation of Sinus Tachycardia
Sinus tachycardia itself does not usually cause symptoms; rather, symptoms are typically related to the underlying cause of the tachycardia, such as pain, fever, or shortness of breath. More sensitive individuals may perceive palpitations or an awareness of their heartbeat.
Sinus tachycardia is an important physiological mechanism that increases cardiac output during infection, fluid loss, or exposure to other stressors. However, like other forms of tachycardia, it can worsen a patient’s condition, particularly in those with underlying heart disease. Tachycardia may reduce cardiac output due to shortened ventricular filling time, decrease oxygen delivery to the myocardium, and impair coronary perfusion.
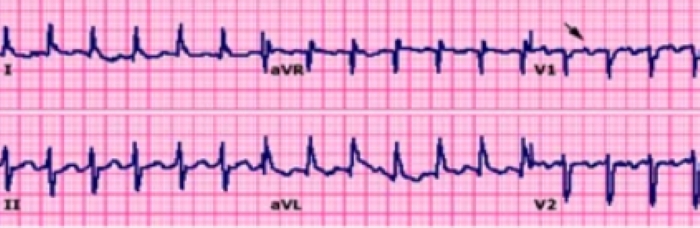
These physiological changes can lead to symptoms such as angina and shortness of breath. The severity of symptoms depends on both the heart rate and the condition of the heart, including the presence of underlying cardiovascular disease. In rare cases, prolonged tachycardia may lead to the development of tachycardia-induced cardiomyopathy (3).Figure 1. Sinus Tachycardia (HR 150 beats/min) ECG

Diagnosis
Tachycardia may initially be suspected by detecting an elevated pulse on palpation or by auscultating an increased heart rate (HR) with a stethoscope. The diagnosis is confirmed by performing an electrocardiogram (ECG). On ECG, sinus tachycardia is characterized by a heart rate exceeding 100 beats per minute and a regular sinus rhythm, with a P wave preceding each QRS complex. At heart rates above 140 beats per minute, differentiation between P and T waves may become difficult (Figure 1) (4).
As a result, sinus tachycardia may occasionally be mistaken for other supraventricular tachycardias. Differentiation can be aided by vagal maneuvers, intravenous medications that temporarily block atrioventricular (AV) nodal conduction, such as adenosine or verapamil, and other agents that slow the sinus rate. These interventions may facilitate ECG interpretation once the rhythm has stabilized.
After sinus tachycardia has been diagnosed, identifying the underlying cause is essential (Table 1). In patients presenting with fever or other signs of infection, routine blood tests are recommended. Measurement of thyroid-stimulating hormone (TSH) should be performed when thyroid dysfunction is suspected, while 24-hour urinary catecholamine and metanephrine testing may be indicated in cases of suspected pheochromocytoma. Additional investigations should be guided by the suspected etiology.
Postural orthostatic tachycardia syndrome (POTS) is diagnosed by assessing heart rate changes in different body positions, typically by measuring HR while the patient is lying, sitting, and standing.
Table 1. Causes of Sinus Tachycardia| Causes of Sinus Tachycardia | Hyperthyroidism | ||
| Fever | Anemia | Pain | |
| Hypovolemia | Hypoxia | Anxiety | |
| Hypotension and shock | Pulmonary embolism | Lack of sleep | |
| Sepsis | Chronic lung diseases | Pheochromocytoma | |
Orthostatic Tachycardia Syndrome Postural Orthostatic Tachycardia Syndrome (POTS) most commonly affects young women without underlying heart disease. Symptoms, including dizziness, fatigue, palpitations, and exercise intolerance, typically occur upon standing. The condition is believed to result from dysfunction of autonomic nervous system regulation. POTS is diagnosed when the heart rate increases by ≥30 beats per minute (≥40 beats per minute in individuals aged 12–19 years) upon standing, in the absence of orthostatic hypotension (defined as a ≥20 mm Hg decrease in systolic blood pressure). The prognosis of POTS is generally favorable, with symptoms resolving spontaneously within one year in approximately one-third of patients. Regular physical activity has been shown to improve symptoms. Fludrocortisone is considered a first-line pharmacological treatment. Pathological Sinus Tachycardia Pathological sinus tachycardia is characterized by a heart rate exceeding 100 beats per minute, with an average daily heart rate greater than 90 beats per minute over a 24-hour period, in the absence of identifiable primary causes such as hyperthyroidism, anemia, or other underlying conditions. Patients with pathological sinus tachycardia typically experience symptoms including palpitations, tremor, shortness of breath, dizziness, and reduced exercise tolerance. The condition is more common in women and may persist for months or even years. Once other potential causes of tachycardia have been excluded, treatment with beta-blockers is recommended. If symptoms persist despite beta-blocker therapy, ivabradine may be prescribed either as monotherapy or in combination with beta-blockers. If adequate symptom control is not achieved, radiofrequency catheter modification of the sinus node may be considered as a final treatment option. However, symptomatic recurrence may occur even after the procedure, sometimes necessitating repeat interventions. In some cases, this may ultimately lead to the need for permanent pacemaker implantation. Beta-Blockers Beta-blockers are considered first-line therapy for pathological sinus tachycardia. Treatment is commonly initiated with 50 mg of extended-release metoprolol, with gradual dose escalation until the desired clinical effect is achieved. High doses are often required to control symptoms, but these may be poorly tolerated. Beta-blockers are most effective when tachycardia is driven by increased sympathetic nervous system activity. In other situations, symptoms may persist despite treatment. Ivabradine In patients with persistent pathological sinus tachycardia, ivabradine is considered a second-line treatment and may be prescribed either alone or in combination with beta-blockers. Ivabradine reduces symptoms in the majority of patients; however, it may increase the risk of atrial fibrillation and is suspected to have teratogenic potential. Patients who develop symptoms suggestive of atrial fibrillation should discontinue the medication and seek medical evaluation. Catheter Ablation After all pharmacological treatment options have been exhausted, patients with pathological sinus tachycardia may be considered for radiofrequency catheter modification of the sinus node. Before the procedure, it is essential to exclude POTS as the underlying cause of tachycardia, as catheter ablation may worsen symptoms in these patients. Although technically challenging, the procedure can achieve success rates of approximately 76–82% when patients are carefully selected. Summary Sinus tachycardia is a rapid heart rhythm (>100 beats per minute) originating from the sinus node. The most common cause is a physiological response to physical exertion or other conditions that activate the sympathetic nervous system and increase catecholamine release, such as fever, pain, hypovolemia, or anxiety. In healthy individuals, sinus tachycardia usually does not cause significant symptoms. However, in patients with underlying cardiovascular disease, it may worsen clinical status and contribute to serious complications. POTS is diagnosed when there is a marked increase in heart rate upon standing without evidence of orthostatic hypotension. The condition is more common in women and often resolves spontaneously over time. Pathological sinus tachycardia is also more frequently observed in women and is characterized by persistently elevated heart rates that cause distressing symptoms. Beta-blockers and ivabradine are the primary treatment options, while catheter modification of the sinus node may be considered in patients who remain symptomatic despite medical therapy.Publication "Internist" No. 3 2020 LITERATURE 1. Control of myocardial oxygen consumption: physiologic and clinical considerations. - PubMed - NCBI. [Online]. Available: https://www.ncbi.nlm.nih.gov/pubmed/4396726. [Accessed: 11-Mar-2020]. 2. Management of tachycardia. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4447058/. [Accessed: 12-Mar-2020]. 3. A case of cardiomyopathy induced by inappropriate sinus tachycardia and cured by ivabradine. - PubMed - NCBI. [Online]. Available: https://www-ncbi-nlm-nih-gov.ezproxy.dbazes.lsmuni.lt/pubmed?term=19572874. [Accessed: 12-Mar-2020]. 4. Sinus tachycardia: Evaluation and management - UpToDate. [Online]. Available: https://www-uptodate-com.ezproxy.dbazes.lsmuni.lt/contents/sinus-tachycardia-evaluation-and-management?search=tachycardia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. [Accessed: 14-Mar-2020]. 5. A prospective, 1-year follow-up study of postural tachycardia syndrome. - PubMed - NCBI. [Online]. Available: https://www-ncbi-nlm-nih-gov.ezproxy.dbazes.lsmuni.lt/pubmed?term=22795533. [Accessed: 14-Mar-2020]. 6. Postural tachycardia syndrome - UpToDate. [Online]. Available: https://www-uptodate-com.ezproxy.dbazes.lsmuni.lt/contents/postural-tachycardia-syndrome?search=tachycardia&topicRef=1074&source=see_link. [Accessed: 14-Mar-2020]. 7. Inappropriate sinus tachycardia: current therapeutic options. - PubMed - NCBI. [Online]. Available: https://www-ncbi-nlm-nih-gov.ezproxy.dbazes.lsmuni.lt/pubmed?term=22143280. [Accessed: 15-Mar-2020]. 8. Inappropriate Sinus Tachycardia - Symptoms and Heart Rate Reduction with Ivabradine: A Pooled Analysis of Prospective Studies. - PubMed - NCBI. [Online]. Available: https://www-ncbi-nlm-nih-gov.ezproxy.dbazes.lsmuni.lt/pubmed?term=29017929. [Accessed: 15-Mar-2020]. 9. Rodríguez-Mañero M, et al. Ablation of Inappropriate Sinus Tachycardia: A Systematic Review of the Literature. JACC Clin Electrophysiol, vol. 3, no. 3, pp. 253–265, 2017, doi: 10.1016/j.jacep.2016.09.014. 10. Scheinman MM, Huang S. The 1998 NASPE Prospective Catheter Ablation Registry. Pacing Clin Electrophysiol, vol. 23, no. 6, pp. 1020–1028, Jun. 2000, doi: 10.1111/j.1540-8159.2000.tb00891.x. |
|||
