
Vitamin D Deficiency: Current Recommendations For Diagnosis, Treatment And Prevention
Vitamin D deficiency affects approximately 50% of the world’s population at some point during life (1). It is estimated that nearly 1 billion people worldwide are affected by vitamin D deficiency in one form or another. This global pandemic of vitamin D hypovitaminosis is associated with changing lifestyles and various environmental factors that reduce time spent outdoors and exposure to sunlight, resulting in decreased vitamin D synthesis in the skin.
Vitamin D deficiency is considered a major public health concern. A lack of this vitamin has been described as an independent risk factor for overall mortality in the global population (2). According to a meta-analysis published in 2007, the use of vitamin D supplements is associated with a clinically significant reduction in mortality (3). Increasing evidence from scientific studies suggests that vitamin D may have beneficial effects in the prevention or treatment of oncological, cardiovascular, autoimmune, infectious diseases, and depression.
This article reviews the classification of vitamin D deficiency, clinical symptoms, diagnostic approaches, treatment, and prevention recommendations for adult patients.
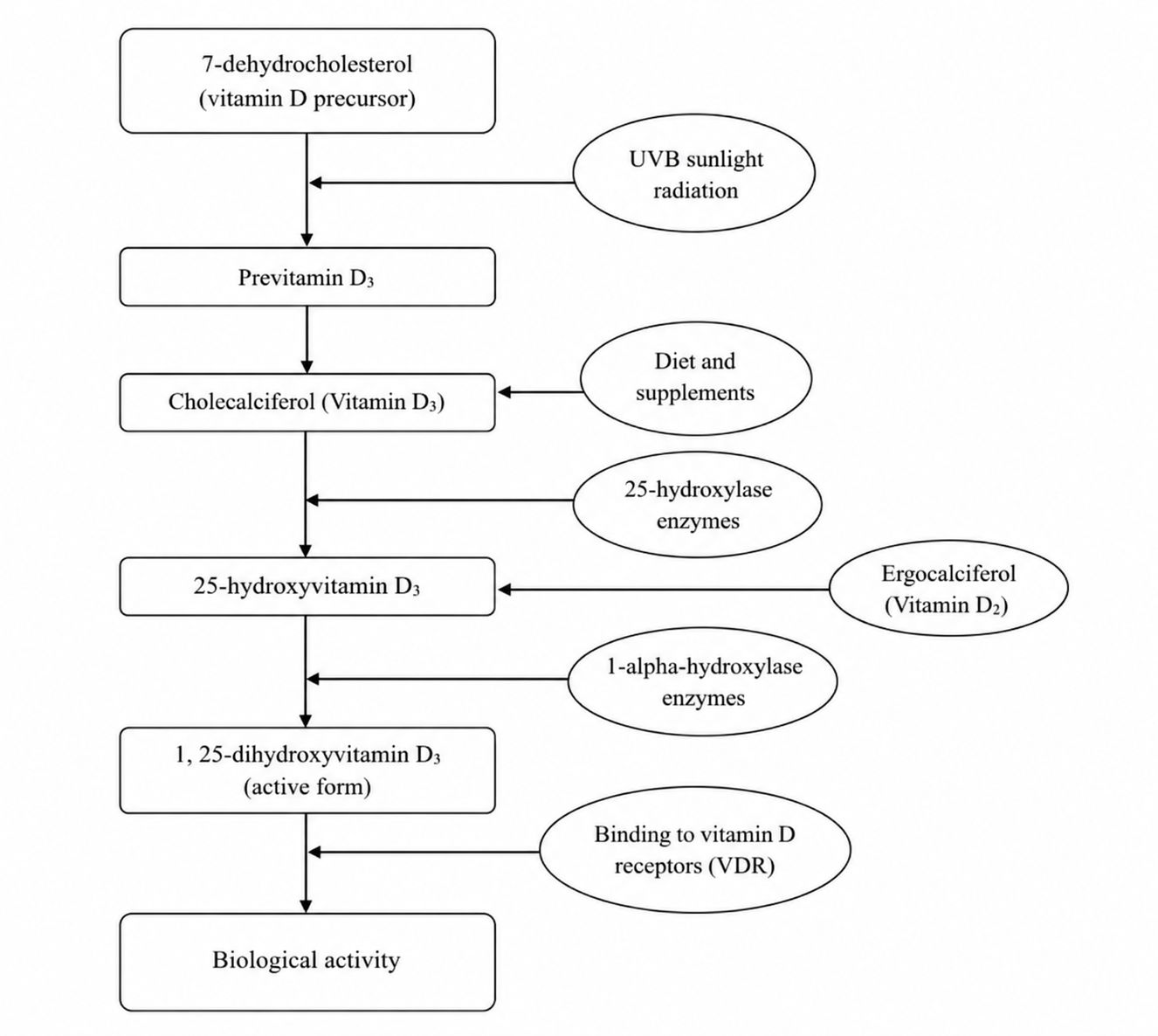
Vitamin D Synthesis and Physiology
Vitamin D belongs to the group of fat-soluble vitamins, which also includes vitamins A, E, and K. There are two forms of vitamin D: vitamin D2 and vitamin D3.
Vitamin D2, also known as ergocalciferol, is obtained from fortified foods, plant-based sources, and dietary supplements. Vitamin D3, also known as cholecalciferol, is obtained from foods such as fatty fish, eggs, cod liver oil, and supplements. Vitamin D3 is also synthesized in human skin under the influence of ultraviolet (UV) rays from sunlight.
Vitamin D Deficiency
The best-known consequences of vitamin D deficiency are rickets in children and osteomalacia in adults. In many developed countries, severe vitamin D deficiency resulting in hypocalcemia and/or hypophosphatemia, rickets, or osteomalacia is relatively rare. However, subclinical mild vitamin D deficiency is frequently detected even in developed countries and is associated with an increased risk of osteoporosis and fractures.
Vitamin D deficiency is also associated with a wide range of additional consequences and manifestations, including skeletal, metabolic, oncological, cardiovascular, autoimmune, infectious diseases, and cognitive impairment.
Causes of Vitamin D Deficiency
Vitamin D deficiency may develop for several reasons, including reduced intake of vitamin D-rich foods, impaired intestinal calcium absorption, insufficient exposure to direct sunlight, accelerated hepatic catabolism, reduced endogenous vitamin D synthesis, and decreased tissue sensitivity to vitamin D.
Groups at Risk of Vitamin D Deficiency
• Elderly individuals: with aging, vitamin D synthesis in the skin decreases, while time spent outdoors and in sunlight is often reduced.
• Individuals living at northern latitudes: these populations receive less sunlight because of geographical factors. In colder climate countries, vitamin D production in the skin is minimal or absent during winter months (4).
• Individuals with dark skin: increased melanin concentration absorbs sunlight and reduces vitamin D synthesis.
• Individuals using sunscreen regularly: during warmer months, the use of sunscreen with SPF 30 may reduce vitamin D synthesis in the skin by more than 95%.
• Obese individuals: a body mass index above 30 is associated with lower vitamin D concentration in the blood (5). Increased subcutaneous fat tissue stores more vitamin D and reduces its release into the bloodstream.
• Individuals who have undergone bariatric gastric bypass surgery: vitamin D absorption may decrease because part of the small intestine responsible for absorption is bypassed.
• Individuals taking medications that accelerate vitamin D catabolism: corticosteroids may reduce calcium absorption and disrupt vitamin D metabolism. Orlistat and cholestyramine may impair absorption of vitamin D supplements, therefore these medications should be taken several hours apart from vitamin D.
• Long-term hospitalized patients or nursing home residents: limited sunlight exposure increases the risk of deficiency.
• Individuals diagnosed with osteoporosis.
• Individuals with malabsorption syndromes of various origins.
For individuals belonging to these risk groups, it is advisable to measure serum vitamin D concentration and prescribe an appropriate vitamin D dose if necessary. Vitamin D concentration should be reassessed after several months to evaluate treatment effectiveness.
Manifestations of Vitamin D Deficiency
The clinical manifestations of vitamin D deficiency depend on both the severity and duration of the deficiency. Many patients with mild or moderate vitamin D deficiency (37.5–50 nmol/L) do not experience specific symptoms. In such cases, serum calcium, phosphorus, and alkaline phosphatase concentrations are usually normal.
In patients with vitamin D concentration between 25–50 nmol/L, elevated parathyroid hormone (PTH) concentration is detected in approximately 40–51% of cases (6). In patients with secondary PTH elevation associated with vitamin D deficiency, the risk of decreased bone density increases (7, 8).
Long-term and severe vitamin D deficiency reduces intestinal absorption of calcium and phosphorus, leading to hypocalcemia followed by secondary hyperparathyroidism, phosphaturia, bone demineralization, osteomalacia in adults, and rickets or osteomalacia in children. Symptoms may include bone pain and tenderness, muscle weakness, and bone fractures.
For patients with vitamin D concentration between 25–50 nmol/L, additional laboratory testing is generally unnecessary.
For patients with vitamin D concentration lower than 25 nmol/L, additional testing is recommended, including assessment of calcium, phosphorus, other electrolytes, alkaline phosphatase, PTH, and serum creatinine concentrations, as well as testing for tissue transglutaminase antibodies to evaluate the possibility of celiac disease.
Extraskeletal Vitamin D Deficiency and Clinical Benefits of Vitamin D Supplements
In addition to its essential role in calcium and bone metabolism, vitamin D regulates numerous other cellular functions. Vitamin D receptors (VDR) are present in nearly all nucleated human cells. Furthermore, at least 10 different tissues express alpha-1 hydroxylase, the enzyme responsible for converting vitamin D into its biologically active form, enabling local paracrine production of this substance.
• Cardiovascular diseases – Vitamin D deficiency is associated with an increased prevalence of coronary heart disease, myocardial infarction, heart failure, and stroke. An analysis of 19 prospective studies found that as serum 25-hydroxyvitamin D (25(OH)D) concentration increased from 20 nmol/L to 60 nmol/L, the risk of cardiovascular disease decreased proportionally (9). This protective effect is believed to be associated with the anti-inflammatory properties of vitamin D.
• Fracture prevention – According to several studies, the use of vitamin D supplements to achieve a target serum vitamin D concentration between 70 nmol/L and 99 nmol/L significantly reduced fracture risk (10–12). However, another study reported that high-dose vitamin D supplementation resulting in persistent 25(OH)D concentration above 100 nmol/L was associated with an increased risk of fractures (13).
• Oncological diseases – Ultraviolet B (UVB) radiation from sunlight is the most important environmental risk factor for skin cancer development. Because sunlight is also the primary source of vitamin D, researchers continue to investigate the role of vitamin D in carcinogenesis. Several studies have suggested possible protective effects of vitamin D against colorectal, breast, and prostate cancer, although these associations have not been sufficiently investigated and reliable evidence remains limited (14, 15).
• Immune system – Vitamin D affects almost all cells of the immune system. Antigen-presenting cells, including dendritic cells, macrophages, and T and B lymphocytes, express VDR. Under certain conditions, the vitamin D endocrine system can regulate multiple aspects of innate and adaptive immunity. The active form of vitamin D, 1,25-dihydroxyvitamin D, inhibits dendritic cell maturation and acts as an immunomodulator that reduces activation of adaptive immunity. Therefore, vitamin D deficiency may theoretically increase the risk of autoimmune diseases (16).
• Infectious diseases – Vitamin D deficiency is associated with an increased risk of upper and lower respiratory tract infections. An analysis of 25 clinical trials demonstrated that vitamin D supplementation slightly reduced the risk of acute upper respiratory tract infections compared with placebo (40.3% vs. 42.2%, CI 0.81–0.96) (17).
• Depression – Vitamin D plays an important role in regulating the synthesis of adrenaline, noradrenaline, and dopamine in the brain, as VDR is present in the adrenal cortex. It is believed that vitamin D may help protect against serotonin and dopamine depletion. Research in this field is still evolving, and precise conclusions are not yet available. Current evidence suggests that vitamin D deficiency may be associated with an 8–14% increased risk of depression.
• Diabetes – Studies have shown that individuals with serum vitamin D concentration above 80 nmol/L had a 43% lower risk of developing type 2 diabetes compared with individuals whose vitamin D concentration was below 45 nmol/L. It is believed that vitamin D improves pancreatic beta-cell function and cellular sensitivity to insulin in type 2 diabetes. In type 1 diabetes, the protective effect of vitamin D is thought to be related to immune system modulation (18).
• Obesity – Obese individuals with type 2 diabetes frequently have reduced serum vitamin D concentration, although the exact mechanisms underlying this association remain unclear. Numerous human studies have demonstrated a relationship between obesity and decreased 25(OH)D concentration (19).
• Pregnancy – Reduced serum vitamin D concentration during the perinatal period may have both short-term consequences, such as preeclampsia, and long-term consequences, including fetal bone disorders and autoimmune or allergic diseases. One study found that insufficient 25(OH)D concentration was associated with increased risk of gestational diabetes, preeclampsia, and low gestational age of the newborn (20).
Determination of Vitamin D Concentration in Serum
Vitamin D status is assessed by measuring serum 25(OH)D, also known as calcidiol. Most laboratories measure total serum 25(OH)D concentration, although some separately determine vitamin D2 and D3 values. Clinically, the most important parameter is total serum 25(OH)D concentration.
Measured serum 25(OH)D levels may vary depending on the laboratory testing method used, and assay variability remains one of the most important issues in establishing an international standard for vitamin D testing (21, 22). Since 2010, an international Vitamin D standardization program has been coordinated by the National Institute of Standards and Technology, Ghent University, and the Centers for Disease Control and Prevention (23).
The most accurate vitamin D concentration measurements are obtained using liquid chromatography with tandem mass spectrometry or similar high-performance liquid chromatography methods calibrated according to National Institute of Standards and Technology standards (24, 25).
Criteria for Determining the Optimal Level of 25(OH)D
Several criteria are used to determine the optimal serum 25(OH)D concentration, including maximal suppression of parathyroid hormone (PTH) by vitamin D and adequate renal production of 1,25-dihydroxyvitamin D. These processes ensure sufficient intestinal calcium absorption and maintenance of normal calcium concentration.
• Maximal PTH suppression – When serum 25(OH)D concentration decreases, intestinal calcium absorption also declines, leading to reduced calcium concentration in the blood. As a compensatory response, serum PTH concentration increases, stimulating conversion of 25(OH)D into 1,25-dihydroxyvitamin D in order to maintain calcium absorption in the intestines. Adequate PTH suppression and normal kidney function are believed to occur when serum vitamin D concentration exceeds 50 nmol/L.
• Reduced substrate conversion – A decrease in serum 25(OH)D concentration also reduces conversion into 1,25-dihydroxyvitamin D, even in the presence of sufficient PTH concentration. This results in impaired intestinal calcium absorption. Studies have shown that these processes begin when serum 25(OH)D concentration falls to approximately 11 nmol/L (26, 27).
Normal Vitamin D Levels and Deficiency Prevention
According to various authors, the normal serum vitamin D concentration ranges from 50–100 nmol/L to 75–125 nmol/L. In general, vitamin D concentration is considered adequate when it reaches 75–100 nmol/L.
The Endocrine Society, the National Osteoporosis Foundation, and the American Geriatrics Society recommend maintaining a minimum serum vitamin D concentration of 75 nmol/L to reduce fracture risk (28). Currently, there is no universally established upper safe limit for serum vitamin D concentration. However, evidence suggests that concentrations above 125 nmol/L may be associated with increased fracture risk and higher mortality risk for certain cancers, including pancreatic and prostate cancer.
For adults who cannot be adequately exposed to sunlight, a daily intake of 600–800 IU of vitamin D is recommended. The recommended daily dose for children aged 1–18 years, adults up to 70 years of age, and pregnant women is 600 IU.
Clinically significant vitamin D deficiency is frequently diagnosed in older adults who spend most of their time indoors and in other high-risk groups, often requiring higher daily vitamin D doses. For individuals older than 70 years, a daily intake of 800 IU is recommended. The American Geriatrics Society and the National Osteoporosis Foundation recommend slightly higher doses, at least 800–1,000 IU daily, for individuals older than 65 years (29).
Treatment of Vitamin D Insufficiency
The amount of vitamin D required for effective treatment of vitamin D insufficiency depends on baseline 25(OH)D concentration, vitamin D absorption capacity, hepatic conversion efficiency, and certain genetic factors.
For patients with severe vitamin D deficiency, higher treatment doses may be required depending on the severity of deficiency and clinical condition.
For patients with 25–50 nmol/L 25(OH)D concentration, 800–1,000 IU of vitamin D daily may be prescribed. In such cases, serum vitamin D concentration should be reassessed after 3 months to determine whether dosage adjustment is necessary.
For patients with 50–75 nmol/L 25(OH)D concentration, 600–800 IU daily is recommended.
In individuals with malabsorption syndromes, vitamin D supplementation and treatment duration depend on the individual’s absorption capacity. In such cases, high doses ranging from 10,000–50,000 IU/day may be prescribed. If vitamin D insufficiency persists despite high-dose treatment, hydroxylated vitamin D metabolites that are more easily absorbed may be administered in combination with light therapy.
Pregnant Women
The exact optimal vitamin D concentration during pregnancy has not been definitively established, but it should not be lower than 50 nmol/L. A daily intake of 600 IU of vitamin D is recommended for all women of reproductive age, pregnant women, and breastfeeding women (30).
Chronic Kidney Disease
For patients with glomerular filtration rate above 30 mL/min and without signs of hyperparathyroidism or hyperphosphatemia, the same vitamin D doses as those used in individuals with normal kidney function may be prescribed.
Primary Hyperparathyroidism
Vitamin D should be administered cautiously in these patients because hypercalcemia and hypercalciuria may develop.
Vitamin D Supplements
Various vitamin D preparations and metabolites may be prescribed for the treatment of vitamin D insufficiency. The recommended dose of vitamin D metabolites depends on the patient’s clinical condition.
• Calcidiol (25(OH)D) – Calcidiol is suitable for patients with liver disease because additional 25-hydroxylation in the liver is unnecessary. Compared with cholecalciferol and ergocalciferol, calcidiol is more hydrophilic and may therefore be prescribed in conditions associated with impaired fat absorption. Calcidiol has a faster onset of action and a half-life of approximately 2–3 weeks, which is shorter than that of vitamin D3. Patients with liver disease may be prescribed 50–200 mcg/day of calcidiol (31).
• Calcitriol (1,25-dihydroxyvitamin D) – Calcitriol is most appropriate for patients with impaired endogenous calcitriol synthesis, such as individuals with chronic kidney disease or kidney failure. It has a rapid onset of action and a short half-life of approximately 6 hours. Because calcitriol use is associated with rapid development of hypercalcemia, serum calcium concentration should be monitored during treatment.
• Dihydrotachysterol – Dihydrotachysterol is a functional equivalent of 1-alpha hydroxyvitamin D and requires 25-hydroxylation in the liver. It has a rapid onset and short duration of action, with therapeutic indications similar to calcitriol.
There is ongoing discussion regarding the most suitable form of vitamin D for supplementation. Currently, cholecalciferol (D3) and ergocalciferol (D2) are the most commonly used forms. Cholecalciferol is generally preferred, while ergocalciferol is prescribed when cholecalciferol is unavailable.
One meta-analysis found that, in patients with comparable degrees of vitamin D deficiency, cholecalciferol increased serum vitamin D concentration more effectively and significantly than ergocalciferol, with an average difference of 15.23 nmol/L (32).
Monitoring of Vitamin D Treatment
When treating vitamin D deficiency with supplementation, serum vitamin D concentration should be reassessed 3–4 months after treatment initiation. If the target concentration is not achieved, the vitamin D dose may need to be increased.
For patients whose serum vitamin D concentration does not increase despite supplementation, testing for tissue transglutaminase antibodies is recommended to evaluate the possibility of celiac disease.
Adverse Effects of Vitamin D Preparations
To avoid vitamin D overdose, it is important to ensure before treatment initiation that the patient is not simultaneously taking other multivitamins or supplements containing vitamin D.
In cases of vitamin D toxicity, the most common manifestations are hypercalciuria and hypercalcemia. However, these symptoms generally occur only when serum 25(OH)D concentration reaches approximately 220 nmol/L (33). The recommended safe upper daily dose of vitamin D is 4,000 IU/day (34).
Importance of Calcium
Individuals aged 19–70 years should consume approximately 1,000 mg of calcium daily from food and supplements combined. Women aged 51–70 years and all individuals older than 71 years require a slightly higher intake of approximately 1,200 mg/day (34).
The maximum recommended calcium intake ranges from 2,000–2,500 mg/day. In specific clinical situations, such as malabsorption syndromes, calcium doses exceeding 4,000 mg/day may be prescribed.
UVB Radiation Exposure
Artificial UVB radiation from tanning beds or similar lamps may effectively increase and/or maintain serum 25(OH)D concentration (35). However, because a safe recommended UVB exposure dose has not been established, artificial UVB radiation sources are generally not recommended for the treatment of vitamin D deficiency (36).
Exceptions may be considered in patients with persistent severe vitamin D deficiency despite treatment with maximal doses of vitamin D preparations (34).
Figure 1.
Summary
• The global pandemic of vitamin D hypovitaminosis is associated with changing lifestyles and various environmental factors that significantly reduce time spent outdoors and exposure to sunlight.
• The use of vitamin D supplementation has been associated with a clinically significant reduction in mortality. Increasing scientific evidence suggests potential beneficial effects of vitamin D in the prevention or treatment of oncological, cardiovascular, autoimmune, infectious diseases, and depression.
• For prevention of vitamin D deficiency, a daily intake of 600 IU of vitamin D is recommended for children aged 1–18 years, adults up to 70 years of age, and pregnant women. Individuals older than 70 years are recommended to consume 800 IU daily.
• In cases of confirmed vitamin D deficiency, vitamin D dosage should be selected individually according to baseline 25(OH)D concentration, vitamin D absorption capacity, hepatic conversion efficiency, and kidney function.
• Cholecalciferol is considered the preferred form of vitamin D supplementation, while ergocalciferol may be prescribed when cholecalciferol is unavailable.
Publication "Internistas" No. 4-5 2018.
References: 1. Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–81. 2. Melamed ML, Michos ED, Post W, Astor B. 25-hydroxyvitamin D levels and the risk of mortality in the general population. Arch Intern Med. 2008;168:1629–37. 3. Autier P, Gandini S. Vitamin D supplementation and total mortality: A meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167:1730–7. 4. Webb AR, Kline L, Holick MF. Influence of season and latitude on the cutaneous synthesis of vitamin D3: exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. J Clin Endocrinol Metab 1988;67:373. 5. Bouillon R, Van Schoor NM, Gielen E, et al. Optimal vitamin D status: a critical analysis on the basis of evidence-based medicine. J Clin Endocrinol Metab 2013; 98:E1283. 6. Valcour A, Blocki F, Hawkins DM, Rao SD. Effects of age and serum 25-OH-vitamin D on serum parathyroid hormone levels. J Clin Endocrinol Metab 2012; 97:3989. 7. Garg MK, Tandon N, Marwaha RK, et al. The relationship between serum 25-hydroxy vitamin D, parathormone and bone mineral density in Indian population. Clin Endocrinol (Oxf) 2014; 80:41. 8. LeBoff MS, Kohlmeier L, Hurwitz S, et al. Occult vitamin D deficiency in postmenopausal US women with acute hip fracture. JAMA 1999; 281:1505. 9. Wang L, Song Y, Manson JE, et al. Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease: a meta-analysis of prospective studies. Circ Cardiovasc Qual Outcomes 2012; 5:819. 10. Dawson-Hughes B, Harris SS, Krall EA, Dallal GE. Effect of calcium and vitamin D supplementation on bone density in men and women 65 years of age or older. N Engl J Med 1997; 337:670. 11. Chapuy MC, Pamphile R, Paris E, et al. Combined calcium and vitamin D3 supplementation in elderly women: confirmation of reversal of secondary hyperparathyroidism and hip fracture risk: the Decalyos II study. Osteoporos Int 2002; 13:257. 12. Trivedi DP, Doll R, Khaw KT. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial. BMJ 2003; 326:469. 13. Sanders KM, Stuart AL, Williamson EJ, et al. Annual high-dose oral vitamin D and falls and fractures in older women: a randomized controlled trial. JAMA 2010; 303:1815. 14. Bauer SR, Hankinson SE, Bertone-Johnson ER, Ding EL. Plasma vitamin D levels, menopause, and risk of breast cancer: dose-response meta-analysis of prospective studies. Medicine (Baltimore) 2013; 92:123. 15. Ahn J, Peters U, Albanes D, et al. Serum vitamin D concentration and prostate cancer risk: a nested case-control study. J Natl Cancer Inst 2008; 100:796. 16. Ponsonby AL, McMichael A, van der Mei I. Ultraviolet radiation and autoimmune disease: insights from epidemiological research. Toxicology 2002; 181-182:71. 17. Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ 2017; 356:i6583. 18. Mathieu C, Gysemans C, Giulietti A, Bouillon R. Vitamin D and diabetes. Diabetologia 2005; 48:1247. 19. Ozfirat Z, Chowdhury TA. Vitamin D deficiency and type 2 diabetes. Postgrad Med J 2010; 86:18. 20. Aghajafari F, Nagulesapillai T, Ronksley PE, et al. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: systematic review and meta-analysis of observational studies. BMJ 2013; 346:f1169. 21. Holmes EW, Garbincius J, McKenna KM. Analytical variability among methods for the measurement of 25-hydroxyvitamin D: still adding to the noise. Am J Clin Pathol 2013; 140:550. 22. Sempos CT, Vesper HW, Phinney KW, et al. Vitamin D status as an international issue: national surveys and the problem of standardization. Scand J Clin Lab Invest Suppl 2012; 243:32. 23. Binkley N, Dawson-Hughes B, Durazo-Arvizu R, et al. Vitamin D measurement standardization: The way out of the chaos. J Steroid Biochem Mol Biol 2017; 173:117. 24. Tai SS, Bedner M, Phinney KW. Development of a candidate reference measurement procedure for the determination of 25-hydroxyvitamin D3 and 25-hydroxyvitamin D2 in human serum using isotope-dilution liquid chromatography-tandem mass spectrometry. Anal Chem 2010; 82:1942. 25. Hoofnagle AN, Eckfeldt JH, Lutsey PL. Vitamin D-Binding Protein Concentrations Quantified by Mass Spectrometry. N Engl J Med 2015; 373:1480. 26. Need AG, O'Loughlin PD, Morris HA, et al. Vitamin D metabolites and calcium absorption in severe vitamin D deficiency. J Bone Miner Res 2008; 23:1859. 27. Lips P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 2001; 22:477. 28. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011; 96:1911. 29. American Geriatrics Society Workgroup on Vitamin D Supplementation for Older Adults. Recommendations abstracted from the American Geriatrics Society Consensus Statement on vitamin D for Prevention of Falls and Their Consequences. J Am Geriatr Soc 2014; 62:147. 30. Institute of Medicine. Report at a Glance, Report Brief: Dietary reference intakes for calcium and vitamin D, released 11/30/2010. (Accessed on December 01, 2010). 31. Basha B, Rao DS, Han ZH, Parfitt AM. Osteomalacia due to vitamin D depletion: a neglected consequence of intestinal malabsorption. Am J Med 2000; 108:296. 32. Tripkovic L, Lambert H, Hart K, et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. Am J Clin Nutr 2012; 95:1357. 33. Gertner JM, Domenech M. 25-Hydroxyvitamin D levels in patients treated with high-dosage ergo- and cholecalciferol. J Clin Pathol 1977; 30:144 34. Institute of Medicine. Report at a Glance, Report Brief: Dietary reference intakes for calcium and vitamin D, released 11/30/2010. (Accessed on December 01, 2010). 35. Datta P, Bogh MK, Olsen P, et al. Increase in serum 25-hydroxyvitamin-D3 in humans after solar exposure under natural conditions compared to artificial UVB exposure of hands and face. Photochem Photobiol Sci 2012; 11:1817. 36. Dawe RS. There are no 'safe exposure limits' for phototherapy. Br J Dermatol 2010; 163:209.
