
Vitamin D and K: Key Questions on Use, Indications, and Dosage
Doc. Aurelija Krasauskienė
Endocrinology Clinic at the Lithuanian University of Health Sciences
Introduction
Why has there been so much discussion about vitamin D and its deficiency recently? It has long been known that children lacking vitamin D develop rickets. This disease was described by Whistler in 1645. In the 19th century, it was linked to a lack of sunlight and was successfully treated by relocating city children to the countryside. In the early 20th century, rickets began to be treated with cod liver oil. The substance found in it was later named vitamin D.
The discovery of the structure of vitamin D and its production in the skin through exposure to sunlight was awarded the Nobel Prize. However, the greatest breakthrough in understanding vitamin D occurred when its mechanism of action in the body was clarified. It was found that for vitamin D to become active, it must undergo internal activation – hydroxylation in the liver and kidneys – and bind to specific vitamin D receptors located in the nuclei of nearly all body cells. It acts as a nuclear transcription factor, promoting cell proliferation and maturation.
This revealed that vitamin D functions not merely as a vitamin – unlike most vitamins involved in specific metabolic processes as coenzymes – but has a much broader role, regulating essential cellular processes such as proliferation and differentiation (1).
This discovery opened the way for research into the wide-ranging effects of vitamin D beyond calcium metabolism. Currently, there is hardly any pathological condition or disease where the impact of vitamin D deficiency on disease progression or recovery has not been studied. In the absence of vitamin D, there is a higher risk of osteoporotic fractures, increased incidence of cancer (especially colorectal and breast cancer), more frequent cardiovascular events, neuropsychiatric disorders, and a more severe course of many autoimmune and infectious diseases.
Although vitamin D may not directly participate in the pathogenesis of these conditions, its deficiency significantly worsens their course and outcomes (2).
The so-called non-skeletal or extraskeletal effects of vitamin D have attracted considerable interest in recent years.
Sources of Vitamin D
● Food. According to the 2007 Lithuanian population nutrition survey, the average intake of vitamin D from food is about 4.9 μg/day (women – 3.9 μg/day, men – 6.3 μg/day) (3). Global recommendations suggest 20 μg/day (1 μg = 40 IU of vitamin D).
● Sunlight. This is the primary source. One minimal erythemal dose (MED) is sufficient to produce an adequate amount of vitamin D – approximately 20,000 IU. One MED is defined as the amount of ultraviolet radiation that causes minimal visible redness of completely fair skin.
● Supplements.
How to Determine Vitamin D Deficiency
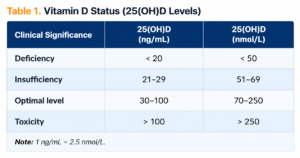
● By measuring the storage form of vitamin D in the body – the circulating form 25(OH)D (calcidiol). This form reflects the total vitamin D obtained from food, supplements, and sunlight. When needed, it is converted in the kidneys into the active form 1,25(OH)₂D.
Measurement of serum 25(OH)D concentration is the basis for determining vitamin D deficiency and its severity, which guides treatment or prevention strategies, including dosage, duration, and regimen (4).
● Target vitamin D levels are defined, although some variability in laboratory results may occur. Officially, up to a 10% variation is acceptable. There is ongoing debate about whether the optimal level should be 70 nmol/L or whether 50 nmol/L may already be insufficient (5).
In cases of vitamin D deficiency, physicians should prescribe high doses and monitor the patient’s condition by periodically measuring blood levels. Once optimal levels are reached, maintenance doses should be continued. In cases of insufficiency, recommended daily doses should be increased or high doses administered occasionally.
Optimal vitamin D levels should be maintained with daily supplementation. If concentrations exceed 125 nmol/L, minimal doses are recommended. During summer, young patients are generally not advised to take vitamin D supplements.
Vitamin D intoxication presents with symptoms of hypercalcemia: kidney damage, constipation, drowsiness, and bradycardia.
Who Should Be Tested for Vitamin D Levels
Routine testing is not recommended for the general population. However, epidemiological studies show that approximately 1 billion people worldwide have suboptimal vitamin D levels. Deficiency is found in 30–100% of individuals depending on age, location, health status, and dietary habits.
Testing is recommended for individuals in risk groups.
Clinical Risk Factors For Vitamin D Deficiency
● Inadequate intake – low dietary intake or insufficient sunlight exposure;
● Digestive disorders – malabsorption of any origin;
● Liver disease and related medications (antiepileptics, glucocorticoids);
● Kidney disease;
● Unexplained muscle weakness or bone pain;
● Laboratory or imaging findings suggesting deficiency (4).
Measures in Case of Vitamin D Deficiency
Before prescribing medication or supplements, it is essential to define the purpose of treatment. Uncertainty regarding treatment goals is the main cause of confusion when selecting doses and formulations.
There is no significant difference between oil-based and water-based vitamin D preparations.
Vitamin D is most commonly prescribed for preventive purposes. According to Central European guidelines (4):
● Infants up to one year – 400–600 IU/day depending on diet;
● Children and adolescents up to 18 years – 600–1,000 IU/day depending on body weight (October to April for those exposed to sunlight, year-round for those with limited exposure);
● Adults and elderly – 800–2,000 IU/day depending on body weight and sunlight exposure (not prescribed in summer for individuals under 65; continuous supplementation recommended for older individuals);
● Pregnant and lactating women – adequate intake before pregnancy; 1,500–2,000 IU/day recommended from the second trimester, maintaining 75 nmol/L levels.
For risk groups:
● Preterm infants – 400–800 IU/day from birth;
● Obese children and adolescents – 1,200–2,000 IU/day (October to April);
● Obese adults (BMI >30) and individuals over 65 – 1,600–2,000 IU/day.
Caution is required when prescribing vitamin D to patients with granulomatous diseases or genetic disorders causing hypercalcemia.
Treatment of Vitamin D Deficiency
Treatment requires significantly higher doses for longer periods. After achieving target levels, maintenance therapy is prescribed.
Adults may receive up to 10,000 IU/day for 3–4 months. Alternative regimens include:
● Every 3 months – 200,000 IU;
● Monthly – 50,000 IU;
● Weekly – 14,000 IU.
A single oral dose of 200,000 IU increases vitamin D levels within 3–4 days. The effect depends on baseline deficiency, body weight, and age.
If 25(OH)D levels are below 50 nmol/L, two doses of 200,000 IU within 3 months are recommended.
Maintenance therapy includes monitoring every 3–6 months and maintaining levels between 75–125 nmol/L. A maintenance dose may include 200,000 IU every 3 months, not exceeding 600,000 IU per year.
Why Is Vitamin K Included in Bone Health Supplements
Cardiologists highlight possible side effects of vitamin D and calcium supplementation. With aging, calcium redistribution occurs – decreasing in bones but accumulating in blood vessel walls.
Vitamin K plays a regulatory role in this process. It participates in the formation of Gla-domain proteins, essential for blood clotting and bone metabolism (osteocalcin, matrix Gla protein, periostin), as well as vascular health (Gas6), reducing calcium deposition in vessels.
Main forms:
● K1 – phylloquinones (plant-based, ~90% of intake);
● K2 – menaquinones (animal-derived, ~10%, also produced by gut flora);
● K3 – menadione (synthetic, potentially toxic).
In vitamin K deficiency, priority is given to blood clotting functions before calcium metabolism. Studies show vitamin K does not increase bone mass but reduces fracture risk.
References
- Rosen C.J. Primer on metabolic bone diseases and disordes of mineral metabolism. 2013, 613–632.
- Camacho P.M., Gharib H., Sizemore G.W. Evidens-based endocrino¬logy. Thirt edition. 2012, 162–164.
- Barzda A., Bartkevičiūtė R., Abaravičius J.A. and others. Suaugusių Lietuvos žmonių faktinės mitybos tyrimas ir vertinimas. Medicinos teorija ir praktika, 2009, T 15 (No. 1), 53–57.
- Pludowski P. et al. Practical guidelines for the supplementation of vitamin D and treatment of deficits in Central Europe. Endocrinologia Polska, 2013, 64 (4), 320–327.
- Ross A.C., Abrams J.E. et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the institute of medicine: what clinicians need to know. Journal of Clinical Endocrinology and Metabolysm, 2011, 53–58.
- Cipriani C., Romagnoli E., Scillitani A., Chiodini I. Effect of a Single Oral Dose of 600,000 IU of Cholecalciferol on Serum Calciotropic Hormones in Young Subjects with Vitamin D Deficiency: A Pros-pective Intervention Study. Journal of Clinical Endocrinology and Metabolysm, 2010, 95 (10), 4771–4777.
- Cesur Y., Caksen H. et al. Comparison of low and hight dose of vit D treatment in nutritional vit D deficienty richetc. Journal of pediatric endocrinology and metabolism, 2011, Vol 16, 1105–1110.
- Kerrie M. et al. Annual high dose oral vitamin D and falls and fractures in older women JAMA, 2010, 303, 18.
- Cockayne S. et al. Vit K and the prevention of fractures.
