
Prolactinoma and Hyperprolactinemia: Diagnosis, Treatment, and Fertility Management
Introduction
Prolactin-secreting adenoma, or prolactinoma, is the most common hormone-secreting pituitary tumor. It is also the only pituitary tumor that can usually be treated effectively with medication alone. For this reason, surgery should generally be avoided unless clearly necessary.
Several important points should be emphasized:
- Hyperprolactinemia is one of the most common causes of hypothalamic-pituitary dysfunction and an important contributor to irregular menstruation and infertility in young women.
- Careful clinical and laboratory evaluation is essential for determining the cause of hyperprolactinemia and selecting appropriate treatment.
- Prolactinoma is the most common cause of pathological hyperprolactinemia.
- Patients with asymptomatic hyperprolactinemia should be tested for macroprolactin, which usually does not require treatment.
- The “hook effect” is a laboratory artifact that may falsely lower measured prolactin levels, complicating differentiation between macroprolactinoma and pseudoprolactinoma.
- Dopamine agonists are effective in approximately 80–90% of hyperprolactinemia cases, reducing both prolactin levels and tumor size. After discontinuation of treatment, normal prolactin levels persist in roughly 20% of patients.
- Surgical treatment is reserved for resistant cases, patients who cannot tolerate medical therapy, or symptomatic pituitary apoplexy.
- Radiotherapy is rarely required and is mainly used to control tumor growth in refractory cases.
- Temozolomide may be considered for aggressive or treatment-resistant prolactinomas that do not respond to dopamine agonists, surgery, or radiotherapy.
- Bromocriptine remains the first-choice dopamine agonist for restoring fertility.
Prolactin Secretion
Prolactin is secreted by lactotroph cells in the anterior pituitary and is primarily regulated by the hypothalamus. Unlike most other anterior pituitary hormones, prolactin secretion is controlled mainly through tonic inhibitory signals from the hypothalamus.
The hypothalamus produces both prolactin-inhibiting factor (PIF) and prolactin-releasing factor (PRF). Dopamine serves as the main PIF, although gamma-aminobutyric acid (GABA) and other substances may also contribute to inhibition of prolactin secretion.
Several substances are believed to function as PRFs, including thyrotropin-releasing hormone (TRH), vasoactive intestinal peptide, oxytocin, galanin, and PHM-27.
Causes of Hyperprolactinemia
The causes of hyperprolactinemia can generally be divided into four major mechanisms, although in some patients the underlying cause remains unidentified.
Dopamine Deficiency in the Hypothalamus
Hypothalamic disorders such as tumors, arteriovenous malformations, or inflammatory diseases including sarcoidosis may reduce dopamine synthesis and release.
Certain medications, such as alpha-methyldopa and reserpine, can also deplete central dopamine stores and contribute to hyperprolactinemia.
Impaired Dopamine Transport
Damage or compression of the pituitary stalk can disrupt dopamine transport from the hypothalamus to the anterior pituitary.
Pituitary or pituitary stalk tumors may impair blood flow or exert pressure effects that interfere with normal hypothalamic-pituitary circulation. As a result, lactotroph cells receive less dopamine inhibition, leading to increased prolactin secretion.
Reduced Sensitivity of Lactotroph Cells to Dopamine
Dopamine receptors are present on pituitary lactotroph cells. Reduced receptor sensitivity may explain why some patients show inadequate suppression of prolactin secretion despite increased endogenous dopamine activity.
However, this mechanism has not been fully clarified because many patients still respond to pharmacological dopamine agonists.
Certain medications act as dopamine receptor antagonists, including:
- phenothiazines (e.g., chlorpromazine),
- butyrophenones (e.g., haloperidol),
- benzamides (e.g., metoclopramide, sulpiride, and domperidone).
These drugs block dopamine receptors and prevent endogenous dopamine from exerting its inhibitory effect on lactotroph cells, resulting in hyperprolactinemia.
Stimulation of Lactotroph Cells
Hypothyroidism can also lead to hyperprolactinemia. Elevated thyrotropin-releasing hormone levels may stimulate prolactin secretion in these patients.
Estrogens also stimulate lactotroph cells and may increase prolactin secretion. In addition, estrogens can enhance the mitotic activity of lactotroph cells, increasing their number within the pituitary.
Hyperprolactinemia may also develop following chest wall injury or irritation.
Clinical Symptoms of Hyperprolactinemia
Clinical manifestations of hyperprolactinemia arise through several mechanisms:
- direct effects of excess prolactin, leading to galactorrhea or hypogonadism;
- structural effects caused by tumor growth, resulting in headaches, visual field defects, or external ophthalmoplegia;
- impaired secretion of other anterior pituitary hormones.
The reported frequency of galactorrhea ranges from 30% to 80%, depending on the physician’s examination technique and the degree of estrogen deficiency.
Interestingly, approximately half of women with galactorrhea have normal prolactin concentrations. Galactorrhea may also disappear when prolactin levels become extremely high, usually above 100 ng/mL (2,000 mU/L). Therefore, galactorrhea is considered an inconsistent sign of hyperprolactinemia.
Women with hyperprolactinemia commonly experience menstrual disturbances, including amenorrhea, oligomenorrhea, and infertility. In some cases, menorrhagia may also occur.
Mild hyperprolactinemia may not produce menstrual abnormalities, but when prolactin concentrations exceed 180 ng/mL (3,600 mU/L), menstrual disturbances are observed in most patients.
In men, symptoms usually appear later than in women and are often related to tumor mass effects, including headaches, visual disturbances, external ophthalmoplegia, or secondary manifestations caused by adrenal or thyroid insufficiency.
Because the disease often progresses silently in men, many patients experience impotence for years before diagnosis. Unlike women, who are more commonly diagnosed with microprolactinomas, men more frequently present with macroprolactinomas and markedly elevated serum prolactin concentrations.
Hyperprolactinemia may occasionally also occur in children and adolescents. Typical manifestations include delayed or arrested puberty, impaired growth, headaches, and visual disturbances. Aggressive prolactinoma variants appear to occur more frequently in children and adolescents than in adults.
Differential Diagnosis
Two major causes of hyperprolactinemia should always be excluded first:
- hypothyroidism,
- medications that reduce dopamine activity or block dopamine receptors.
After excluding these causes and ruling out pituitary damage, the remaining major possibilities include:
- microadenoma,
- macroadenoma,
- non-tumorous disorders.
If imaging studies fail to identify a tumor, the condition is classified as idiopathic hyperprolactinemia.
It is possible that some patients with idiopathic hyperprolactinemia have extremely small microprolactinomas that remain undetectable on imaging studies.
A microadenoma is defined as a pituitary adenoma measuring up to 10 mm in diameter, whereas a macroadenoma exceeds 10 mm.
Microadenomas are typically visualized using magnetic resonance imaging (MRI). In patients with microadenomas, serum prolactin concentrations are usually below 200 ng/mL (4,000 mU/L), while concentrations above this level are more characteristic of macroprolactinomas.
If a patient has a macroadenoma but prolactin levels remain below 200 ng/mL (4,000 mU/L), a non-functioning pituitary adenoma (pseudoprolactinoma) should be considered.
The Hook Effect
Differentiating macroprolactinomas from pseudoprolactinomas may be complicated by laboratory artifacts.
When prolactin is measured using a two-site immunometric assay, extremely high prolactin concentrations may saturate both antibodies in the assay, resulting in falsely low measured prolactin levels. This phenomenon is known as the hook effect.
As a result, patients with very large prolactinomas and extremely elevated prolactin levels — often exceeding 1,000 ng/mL (180,000 mU/L) — may incorrectly appear to have only moderately elevated prolactin levels, such as 30–120 ng/mL (600–2,400 mU/L).
This may lead to the mistaken diagnosis of a non-functioning pituitary adenoma and potentially unnecessary surgery.
To avoid diagnostic errors, prolactin testing should be repeated using diluted serum samples in patients with macroadenomas and unexpectedly low prolactin concentrations.
Macroprolactinemia
Another diagnostic challenge occurs in patients with markedly elevated prolactin concentrations but minimal or absent symptoms of hyperprolactinemia.
The most common circulating form of prolactin is monomeric prolactin, but larger prolactin complexes may also be present in serum. Some of these complexes, particularly macroprolactin, have low biological activity yet may produce falsely elevated prolactin measurements.
This condition is referred to as macroprolactinemia.
Macroprolactinemia should be suspected in patients with elevated serum prolactin levels who lack clinical symptoms associated with hyperprolactinemia.
Polyethylene glycol (PEG) precipitation is considered an effective screening method for detecting macroprolactin. Chromatographic analysis can confirm the diagnosis, although it is expensive and time-consuming and is generally reserved for unclear cases.
Reported prevalence rates of macroprolactinemia vary widely, ranging from 8% to 42% of hyperprolactinemia cases, although some centers report it as relatively uncommon.
Whether macroprolactin possesses significant biological activity remains uncertain. Most patients with macroprolactinemia do not develop symptoms of hyperprolactinemia and therefore usually do not require treatment.
Breast Changes Associated With Prolactin
Women with hyperprolactinemia-associated amenorrhea generally do not develop the breast atrophy typically observed in postmenopausal women or in women with gonadotropin deficiency or primary ovarian insufficiency.
Instead, the breasts and areolae usually remain well developed, and Montgomery glands may appear hyperplastic.
When breast examination is performed correctly, galactorrhea is often detected. Examination involves applying pressure from the periphery of the areola toward the milk ducts and gently compressing and elevating the areola rather than the nipple itself.
However, patients with extremely high prolactin concentrations may still lack galactorrhea.
In men with hyperprolactinemia, gynecomastia is usually absent, although galactorrhea may occur even in the presence of a normal male chest.
Galactorrhea in men is relatively uncommon, occurring in fewer than 30% of cases. Nevertheless, when galactorrhea occurs together with a pituitary lesion, prolactinoma becomes a highly likely diagnosis.
Hyperprolactinemic Hypogonadism
The mechanisms underlying hypogonadism in hyperprolactinemia are not fully understood.
Recent animal studies suggest that hyperprolactinemia reduces kisspeptin activity, which normally regulates pulsatile gonadotropin-releasing hormone secretion.
Men typically exhibit reduced testosterone levels, although testosterone may occasionally remain within normal limits. Women may develop hypoestrogenism accompanied by anovulation.
Clinical manifestations of hyperprolactinemia in women differ from those seen after menopause because breast atrophy is usually absent and gonadotropin concentrations are not elevated.
Suppression of Gonadal Function in Hyperprolactinemia
Hyperprolactinemia suppresses gonadal function through several mechanisms. Excess prolactin inhibits gonadotropin secretion, interferes with progesterone synthesis, may stimulate adrenal androgen production, and reduces the responsiveness of the gonads to gonadotropin hormones.
Through feedback effects on the hypothalamus, prolactin causes inappropriately low secretion of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). It also disrupts the pulsatile secretion of LH, which is essential for normal gonadal function and reproductive health.
Imaging Studies of the Pituitary Gland
Magnetic resonance imaging (MRI) is the preferred method for evaluating pituitary anatomy.
MRI allows detailed visualization of:
- the pituitary gland,
- pituitary tumors,
- the pituitary stalk,
- the optic chiasm,
- cavernous sinuses,
- surrounding brain structures.
MRI can also identify aneurysms within the circle of Willis and accurately determine tumor size, invasion, and anatomical relationships with nearby structures.
Sellar cysts and herniations may also be visualized.
If MRI cannot be performed, computed tomography (CT) may provide additional information, although its resolution for evaluating the sellar region and optic chiasm is inferior to MRI.
Conventional skull radiography has very limited value because it primarily visualizes bony structures rather than soft tissue abnormalities.
Treatment of Hyperprolactinemia
Treatment strategy depends on several factors, including:
- the patient’s symptoms,
- tumor size,
- the natural course of microprolactinomas and macroprolactinomas,
- fertility and pregnancy plans,
- patient preference.
Currently, medical therapy with dopamine agonists (DAs) is considered the gold standard treatment for both microprolactinomas and macroprolactinomas.
Transsphenoidal pituitary surgery is generally reserved for patients who are resistant to dopamine agonists or unable to tolerate medical therapy.
In patients undergoing surgery for microadenomas, normal prolactin levels are achieved in approximately 80% of cases. However, even when surgery is performed by highly experienced neurosurgeons, recurrence of hyperprolactinemia occurs in roughly 25% of patients within five years.
Surgical outcomes are generally less favorable in patients with macroprolactinomas, particularly when tumors are large or invasive.
Radiotherapy is now used only rarely and is mainly reserved for aggressive macroadenomas that remain resistant to both medical and surgical treatment.
Medical Therapy With Dopamine Agonists
The first dopamine agonist widely used in clinical practice was bromocriptine, a peptide-derived compound with more than 40 years of clinical experience.
Bromocriptine offers advantages over dopamine itself and older oral agents such as levodopa because of its longer duration of action.
Its mechanism of action resembles that of dopamine: bromocriptine stimulates D2 dopamine receptors located on prolactin-secreting lactotroph cells in the pituitary gland.
Activation of these receptors suppresses both prolactin synthesis and prolactin secretion.
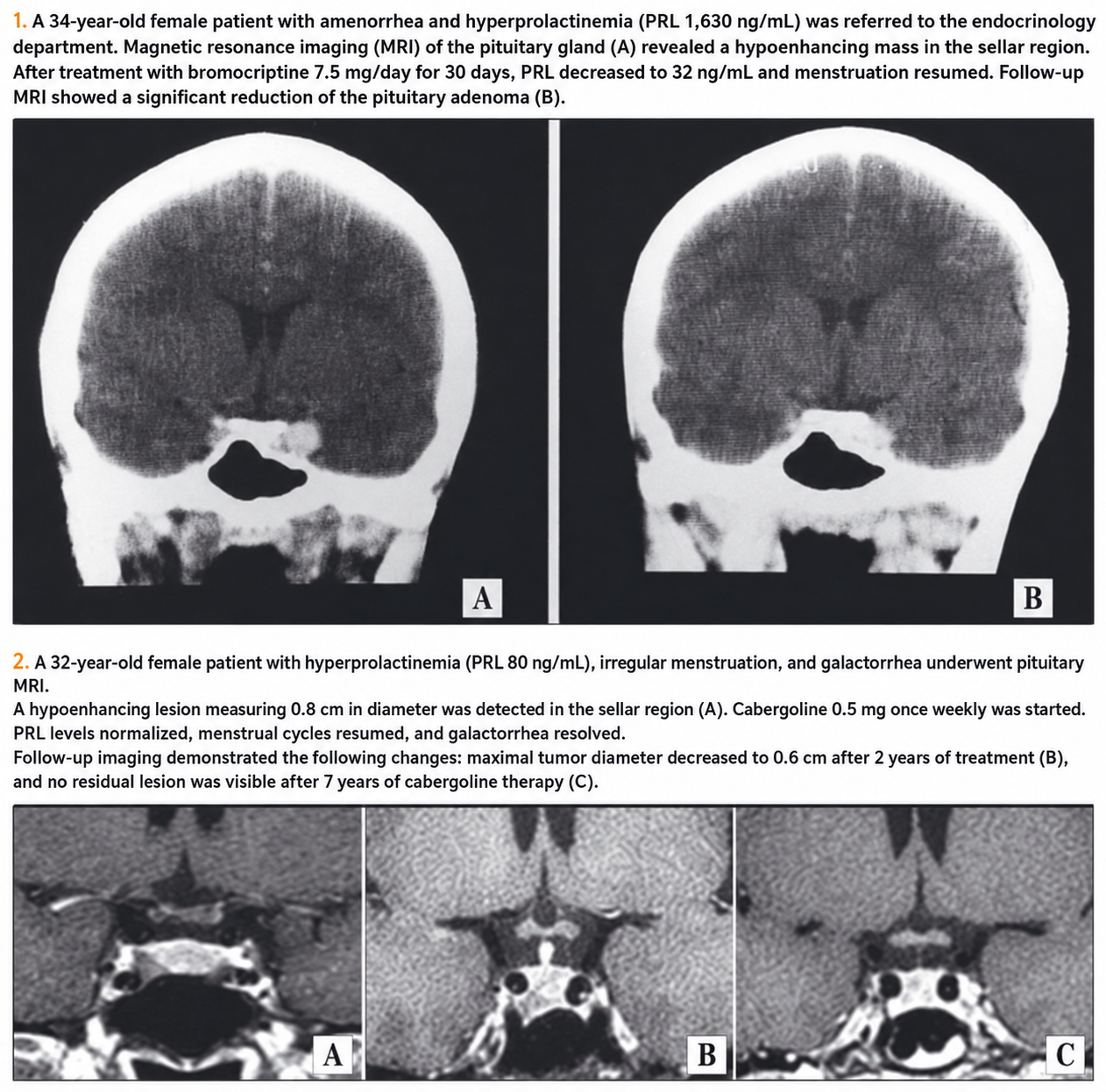
Slide 1. A successful case of prolactinoma treatment with bromocriptine is presented. Later, additional dopamine agonists were developed, including pergolide mesylate, quinagolide, and cabergoline.
Cabergoline has a particularly long half-life and is therefore administered only once or twice weekly. The usual weekly dose ranges from 0.5 to 2.0 mg, although higher doses may be required in resistant cases. Compared with bromocriptine, cabergoline is generally better tolerated, which improves patient adherence to treatment.
Cabergoline is currently considered the first-line therapy for prolactinomas, except in patients planning pregnancy in the near future.
One study involving 459 women with hyperprolactinemia and amenorrhea compared bromocriptine (2.5–5 mg twice daily) with cabergoline (0.5–1.0 mg twice weekly).
Stable normalization of prolactin levels was achieved in:
- 83% of patients treated with cabergoline,
- 59% of patients treated with bromocriptine.
Ovulatory cycles or pregnancy occurred in:
- 72% of patients in the cabergoline group,
- 52% of patients in the bromocriptine group.
Only 3% of patients receiving cabergoline discontinued treatment because of adverse effects, compared with 12% in the bromocriptine group.
Tumor size reduction of at least 50% was observed in:
- 93% of cabergoline-treated patients,
- 64% of bromocriptine-treated patients (Slide 2).
These findings demonstrate that dopamine agonist therapy can rapidly reduce symptoms caused by tumor mass and may help avoid surgical decompression.
Surgical treatment of large prolactin-secreting tumors is often less successful, with normalization of serum prolactin levels and restoration of gonadal function occurring in fewer than 20% of patients. Therefore, medical therapy remains an important and effective treatment strategy for large prolactinomas.
Adverse Effects
Adverse effects of dopamine agonists usually occur at the beginning of treatment and often diminish over time.
Rapid dose escalation or initiation with high doses may cause:
- dizziness,
- nausea,
- orthostatic hypotension.
To reduce these adverse effects, dopamine agonists should be taken with food, preferably before bedtime after a light snack.
Cabergoline and pergolide have been associated with an increased risk of valvular heart disease in patients with Parkinson’s disease. Dopamine agonists stimulate serotonin 5-HT2B receptors located in cardiac valves and chordae tendineae.
Activation of these receptors may promote fibroblast proliferation and lead to valvular insufficiency, particularly involving the tricuspid and mitral valves.
However, the doses used in Parkinson’s disease (approximately 3 mg/day of cabergoline) are substantially higher than those typically prescribed for hyperprolactinemia.
Among 17 observational studies evaluating valvular risk during cabergoline treatment for hyperprolactinemia, only one reported a moderate increase in tricuspid regurgitation.
There is ongoing debate regarding the necessity of routine echocardiography during cabergoline therapy. Nevertheless, echocardiographic evaluation is generally recommended before initiating dopamine agonist treatment and periodically during follow-up.
Because of concerns regarding valvular toxicity, pergolide was withdrawn from the market.
Does Hyperprolactinemia Recur After Discontinuation of Dopamine Agonists?
One limitation of medical treatment for prolactinomas is the need for long-term therapy.
In many patients, discontinuation of bromocriptine leads to recurrence of hyperprolactinemia and tumor regrowth, particularly after shorter treatment durations.
According to retrospective data:
- 25.8% of patients with microprolactinomas,
- 15.9% of patients with macroprolactinomas
maintained normal prolactin levels after discontinuing long-term bromocriptine therapy.
Median follow-up duration after discontinuation was:
- 44 months for microprolactinomas,
- 47 months for macroprolactinomas.
In studies evaluating cabergoline, treatment was discontinued after normalization of prolactin levels and at least a 50% reduction in tumor size or complete tumor disappearance. Patients were followed for at least two years after discontinuation.
Normal serum prolactin levels persisted in:
- 76% of patients with idiopathic hyperprolactinemia,
- 70% of patients with microprolactinomas,
- 60% of patients with macroprolactinomas.
However, later meta-analyses involving 743 patients from 19 studies did not confirm a statistically significant superiority of cabergoline over bromocriptine.
According to pooled results:
- remission occurred in 32% of patients with idiopathic hyperprolactinemia,
- 21% of patients with microprolactinomas,
- 16% of patients with macroprolactinomas.
The likelihood of successful remission appears to increase when dopamine agonist therapy is continued for at least two years.
Although the exact mechanisms underlying prolactinoma remission remain unclear, spontaneous changes in the natural course of the disease may also contribute.
Periodic attempts to discontinue dopamine agonist therapy are recommended, especially in patients with normalized prolactin levels and significant tumor shrinkage.
DA-Resistant Prolactinomas
Approximately 15% of prolactinomas are resistant to dopamine agonist (DA) therapy. The main mechanism underlying resistance is altered expression of D2 dopamine receptors within the tumor.
If a patient initially responds to treatment but later develops resistance, pituitary carcinoma should be considered and excluded.
Treatment options for DA-resistant prolactinomas include:
- surgery,
- radiotherapy,
- chemotherapy with agents such as temozolomide.
Surgical treatment is generally more successful in microadenomas and non-invasive macroadenomas, achieving remission in approximately:
- 74.7% of microadenomas,
- 34% of macroadenomas.
Radiotherapy is typically reserved for aggressive tumors that cannot be adequately controlled with surgery or medical therapy.
Temozolomide has shown effectiveness in the treatment of aggressive pituitary adenomas, particularly prolactin-secreting adenomas and pituitary carcinomas.
Pregnancy and Bromocriptine
Successful treatment of hyperprolactinemia and prolactinomas in women often restores fertility.
When managing pregnancy in patients with prolactinomas, two major concerns must be considered:
- the risk of tumor enlargement during pregnancy,
- the potential teratogenic effects of bromocriptine or other medications on the fetus.
Although the likelihood of tumor growth during pregnancy is generally low, it remains clinically significant.
The risk of adenoma enlargement is more difficult to assess in individual patients. In women with untreated or non-irradiated microadenomas, reported recurrence or growth rates during pregnancy range from 15.5% to 41%.
The risk does not appear to depend on prior bromocriptine treatment before conception. However, the likelihood of tumor growth may increase in women who required ovulation induction with exogenous gonadotropins or clomiphene for infertility treatment.
In clinical practice, pregnancy-related complications are relatively uncommon because most women with hyperprolactinemia are diagnosed with microprolactinomas.
Before pregnancy, patients should undergo:
- endocrine evaluation,
- neuroradiological assessment,
- neuro-ophthalmological examination.
In patients with microadenomas, the likelihood of significant pituitary enlargement during pregnancy is low. Monitoring every three months during pregnancy is generally recommended.
In patients with macroadenomas, especially those extending beyond the sella turcica, dopamine agonist therapy is usually continued.
If prolactin levels normalize and the adenoma decreases in size and remains confined to the sella turcica for at least one year before pregnancy, dopamine agonists may be discontinued with careful monitoring for tumor regrowth.
If significant tumor enlargement occurs, pituitary surgery or induction of labor may become necessary.
In cases of pituitary apoplexy during pregnancy, high-dose dexamethasone is administered to reduce clinical symptoms. In cases of premature delivery, dexamethasone may also help reduce the risk of fetal respiratory distress syndrome.
In the United States, bromocriptine remains the only medication approved by the US Food and Drug Administration (FDA) for restoring fertility and treating hyperprolactinemia during pregnancy.
Presentation of more data and safety information about Cabergoline - the frequency of miscarriages, premature births, multiple pregnancies, congenital malformations in studies does not differ from Bromocriptine and the general population frequency. However, until studies are of sufficient size, Cabergoline is not recommended for those wishing to conceive or during pregnancy. The use of Quinagolide is associated with abortions and malformations.
Summary
DA successfully cures hyperprolactinemic hypogonadism without the risk of pituitary insufficiency, thus overcoming infertility successfully. DA therapy is effective not only for patients with microadenomas but also for many patients with macroadenomas - reducing their size. In addition, there is evidence that after long-term drug use, they can be discontinued.
Surgical treatment, radiotherapy, and chemotherapy drugs such as Temozolomide are reserved for resistant and aggressive cases of the disease.
Journal INTERNIST supplement on CURRENT ISSUES IN ENDOCRINE DISEASES,
