
Diabetes and Dementia: The Hidden Role of Hypoglycemia
Introduction
Recently, scientific research has shown a consistent decrease in morbidity and mortality from cardiovascular diseases, previously considered the main cause of death among patients with diabetes mellitus (DM) (1). This is a significant positive consequence of various risk factors related to DM, early diagnosis, and control (2–5). Intensive control of risk factors in the future should not only improve the quality of life of people with DM but also prolong their lifespan (6). While a decrease in cardiovascular complications has been observed, the prevalence of other complications often associated with DM, such as neurodegenerative disorders, is constantly increasing, along with the clinical significance of these disorders (7). Previous studies have found that DM through various mechanisms has a significant impact on the development of dementia and cognitive disorders (7–8). Hypoglycemia is very important, often occurring due to strict DM control, directly increasing the risk of developing cognitive disorders, negatively affecting the clinical condition and prognosis of diabetics (9). In this article, we will discuss the factors leading to dementia and cognitive dysfunction in patients with DM and hypoglycemia.Relationship Between DM and Dementia
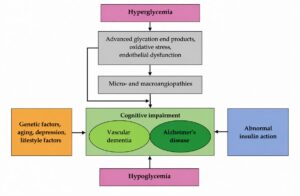
Several epidemiological studies have observed an increased risk of dementia and cognitive disorders among patients with DM. In a cross-sectional study conducted in Germany, the risk of significant cognitive function decline in the group of individuals with DM was 1.82 times higher, and in undiagnosed and untreated diabetics, it was 2.12 times higher compared to patients without DM (10). In one study comparing individuals with and without DM, the relative risk of Alzheimer's disease was 1.56 (95% CI 1.41–2.66), and the relative risk of vascular dementia was 2.27 (95% CI 1.94–2.66) (11). In a study conducted in Korea, the relative risk of Alzheimer's disease was 1.4 (95% CI 1.1–1.7), and the relative risk of vascular dementia was 2.8 (95% CI 2.0–3.9) when comparing individuals with and without DM (12). It is known that DM is a mortality-increasing factor among patients with dementia. In a retrospective study, the mortality of patients with DM was 1.9 times higher than that of individuals without DM (95% CI 1.3–2.9) (13). Although the exact mechanism of DM leading to the development of dementia and cognitive disorders is not known, several significant factors have been identified (Figure 1). DM can create favorable conditions for the development of dementia, one of which is when the threshold for amyloid plaques in brain tissue decreases (14). In addition, DM-related microvascular ischemic stroke risk, which increases the risk of vascular dementia, is a factor (15–16). Regardless of the development of cerebrovascular diseases, insulin resistance and hyperinsulinemia are among the most important factors in the development of dementia (17). Studies have shown that the accumulation of beta-amyloid and hyperphosphorylation of tau protein are important in this process (18). Advanced glycation end products induced by hyperglycemia promote glycation of beta-amyloid and tau protein, which is associated with the development of dementia (19). It has been found that oxidative stress and chronic low-grade inflammation, which are important in type 2 DM, are related to beta-amyloid metabolism (8).Figure 1. Factors contributing to dementia and cognitive disorders in DM
 Relationship Between Hypoglycemia and Dementia
Relationship Between Hypoglycemia and Dementia
The causes and manifestations of hypoglycemia vary with age, but it is a relatively common clinical condition among patients with type 2 DM. According to data from a meta-analysis conducted in 2015, the development of mild or moderate-severe hypoglycemia in patients with type 2 DM reached 19 episodes per year, while severe hypoglycemia reached 0.8 episodes per year per patient (20). In a cohort study of the Korean National Diabetes Program (KNDP), the frequency of hypoglycemia among patients with DM up to 50 years old was 3.72 cases per 1,000 people per year, gradually increasing with age and reaching 25.75 cases per 1,000 people per year in the elderly group (21).
Research has shown the negative impact of hypoglycemia on the clinical condition and prognosis of patients with DM (9, 11, 22). It has also been shown that increased medical expenditure leads to increased costs and burden on the healthcare system (21). In older patients, episodes of hypoglycemia are more frequent due to comorbidities, inadequate nutrition, extensive use of various medications, long duration of illness, and kidney and liver dysfunction. Changes in key cognitive functions after episodes of hypoglycemia can trigger the development of hypoglycemic encephalopathy. It is known that recurrent hypoglycemia contributes to cognitive disorders and that this relationship is important for the development of dementia both as a cause and a consequence (23–24).
In a retrospective study involving 16,667 elderly patients with CD, the risk of dementia after a single severe hypoglycemia episode (requiring hospitalization or emergency room visit) increased to 26% (1.80; 95% CI 1.10–1.49), after two episodes to 80% (1.94; 95% CI 1.37–2.36), and after three or more episodes to 94% (1.94; 95% CI 1.42–2.64) (22). In another cohort study where elderly diabetic patients with dementia or cognitive impairments were examined, patients were significantly more likely to be admitted to healthcare facilities due to hypoglycemia compared to those without these conditions (13). The relationship between hypoglycemia and dementia was investigated in the KNDP subcohort study (9). The study included 1,957 individuals aged 60 and older, who had previously participated in the KNDP cohort study and had no history of severe hypoglycemia. The average follow-up time for patients was 3.4 years, during which dementia occurred at a rate of 7.5 cases per 1,000 individuals per year. The risk of dementia was 2.689 times higher for individuals who experienced severe hypoglycemia (95% CI 1.080–6.694) compared to those who did not experience severe hypoglycemia (9). Furthermore, as the number of hypoglycemia episodes increases, the risk of dementia significantly rises.
How to Reduce the Frequency of Hypoglycemia in Patients with CD?
Unfortunately, there are no randomized controlled trials determining the best hypoglycemia prevention strategy to avoid dementia in patients with CD. However, data from previous studies suggest that hypoglycemia prevention could be crucial for preventing dementia and cognitive impairments. Various treatment guidelines suggest that strict glycemic control may not be beneficial for frail elderly patients, and target blood glucose levels should be set more flexibly (25). Tailoring flexible glycemic control to elderly patients with CD who are at higher risk of hypoglycemia could have a positive impact on clinical outcomes and prognosis. For CD patients at high risk of hypoglycemia, regular diet and a healthy lifestyle also have a positive effect (23). When choosing diabetes medications, it would be beneficial to opt for drugs with a low risk of hypoglycemia (26–27). Patients with multiple comorbidities who take various medications are at increased risk of drug interactions, so reducing the number of medications should be considered (27). Recently, significant attention has been given to information processing and communication technologies to improve the control of chronic diseases, including CD. Studies have shown that using the latest technologies can enhance CD management, improve patients' glycemic levels, and contribute to complication prevention (28).Conclusion
Although specific mechanisms are not fully understood, CD is a significant factor in the development of dementia and cognitive impairments. Several factors have been identified that can contribute to the development of dementia in patients with CD. Hypoglycemia, often occurring during CD treatment and significantly impacting the development of dementia and cognitive impairments when not properly corrected, is particularly important. Individualized treatment for patients with CD, considering the influence of comorbidities and the complexity of clinical situations in elderly patients, could help reduce the frequency of hypoglycemia and have a positive impact on reducing adverse clinical outcomes, including dementia.Publication "Internistas" No. 3 2018
References
1. Huskins WC, Huckabee CM, O'Grady NP, Murray P, Kopetskie H, Zimmer L, et al. Intervention to reduce transmission of resistant bacteria in intensive care. N Engl J Med 2011;364:1407–1418. 2. Action to Control Cardiovascular Risk in Diabetes Study Group. Gerstein HC, Miller ME, Byington RP, Goff DC Jr, Bigger JT, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 2008;358:2545–2559. 3. ADVANCE Collaborative Group. Patel A, MacMahon S, Chalmers J, Neal B, Billot L, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008;358:2560–2572. 4. Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 2009;360:129–139. 5. Riddle MC, Ambrosius WT, Brillon DJ, et al. Epidemiologic relationships between A1C and all-cause mortality during a median 3.4-year follow-up of glycemic treatment in the ACCORD trial. Diabetes Care 2010;33:983–990. 6. Lutgers HL, Gerrits EG, Sluiter WJ, et al. Life expectancy in a large cohort of type 2 diabetes patients treated in primary care (ZODIAC-10). PLoS One 2009;4:e6817. 7. Ott A, Stolk RP, van Harskamp F, Pols HA, Hofman A, Breteler MM. Diabetes mellitus and the risk of dementia: the Rotterdam study. Neurology 1999;53:1937–1942. 8. Sims-Robinson C, Kim B, Rosko A, Feldman EL. How does diabetes accelerate Alzheimer disease pathology? Nat Rev Neurol 2010;6:551–559. 9. Chin SO, Rhee SY, Chon S, et al. Hypoglycemia is associated with dementia in elderly patients with type 2 diabetes mellitus: an analysis based on the Korea National Diabetes Program Cohort. Diabetes Res Clin Pract 2016;122:54–61. 10. Fink A, Buchmann N, Tegeler C, et al. Physical activity and cohabitation status moderate the link between diabetes mellitus and cognitive performance in a community-dwelling elderly population in Germany. 2017; PLoS ONE 12(10): e0187119. 11. Gudala K, Bansal D, Schifano F, Bhansali A. Diabetes mellitus and risk of dementia: a meta-analysis of prospective observational studies. J Diabetes Investig 2013;4:640–650. 12. Kimm H, Lee PH, Shin YJ, et al. Mid-life and late-life vascular risk factors and dementia in Korean men and women. Arch Gerontol Geriatr 2011;52:e117–e122. 13. Zilkens RR, Davis WA, Spilsbury K, Semmens JB, Bruce DG. Earlier age of dementia onset and shorter survival times in dementia patients with diabetes. Am J Epidemiol 2013;177:1246–1254. 14. Schneider JA, Arvanitakis Z, Bang W, Bennett DA. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology 2007;69:2197–2204. 15. Vermeer SE, Prins ND, den Heijer T, Hofman A, Koudstaal PJ, Breteler MM. Silent brain infarcts and the risk of dementia and cognitive decline. N Engl J Med 2003;348:1215–1222. 16. Launer LJ, Hughes TM, White LR. Microinfarcts, brain atrophy, and cognitive function: the Honolulu Asia Aging Study Autopsy Study. Ann Neurol 2011;70:774–780. 17. De Felice FG, Lourenco MV, Ferreira ST. How does brain insulin resistance develop in Alzheimer's disease? Alzheimers Dement 2014;10 1 Suppl:S26–S32. 18. Park CR. Cognitive effects of insulin in the central nervous system. Neurosci Biobehav Rev 2001;25:311–323. 19. Deane R, Du Yan S, Submamaryan RK, et al. RAGE mediates amyloid-beta peptide transport across the blood-brain barrier and accumulation in brain. Nat Med 2003;9:907–913. 20. Edridge CL, Dunkley AJ, Bodicoat DH, et al. Prevalence and Incidence of Hypoglycaemia in 532,542 People with Type 2 Diabetes on Oral Therapies and Insulin: A Systematic Review and Meta-Analysis of Population Based Studies. 2015; PLoS ONE 10(6): e0126427. 21. Rhee SY, Hong SM, Chon S, et al. Hypoglycemia and medical expenses in patients with type 2 diabetes mellitus: an analysis based on the Korea National Diabetes Program Cohort. PLoS One 2016;11:e0148630. 22. Whitmer RA, Karter AJ, Yaffe K, Quesenberry CP Jr, Selby JV. Hypoglycemic episodes and risk of dementia in older patients with type 2 diabetes mellitus. JAMA 2009;301:1565–1572. 23. Abdelhafiz AH, Rodriguez-Manas L, Morley JE, Sinclair AJ. Hypoglycemia in older people: a less well recognized risk factor for frailty. Aging Dis 2015;6:156–167. 24. Bruce DG, Davis WA, Casey GP, et al. Severe hypoglycaemia and cognitive impairment in older patients with diabetes: the Fremantle Diabetes Study. Diabetologia 2009;52:1808–1815. 25. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015;38:140–149. 26. Mallery LH, Ransom T, Steeves B, Cook B, Dunbar P, Moorhouse P. Evidence-informed guidelines for treating frail older adults with type 2 diabetes: from the Diabetes Care Program of Nova Scotia (DCPNS) and the Palliative and Therapeutic Harmonization (PATH) program. J Am Med Dir Assoc 2013;14:801–808. 27. Mathieu C, Bollaerts K. Antihyperglycaemic therapy in elderly patients with type 2 diabetes: potential role of incretin mimetics and DPP-4 inhibitors. Int J Clin Pract Suppl 2007;(154):29–37. 28. Lim S, Kang SM, Shin H, et al. Improved glycemic control without hypoglycemia in elderly diabetic patients using the ubiquitous healthcare service, a new medical information system. Diabetes Care 2011;34:308–313.
